





Which Came First—Better Education or Better Health?
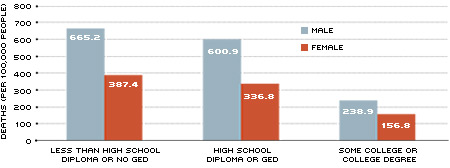
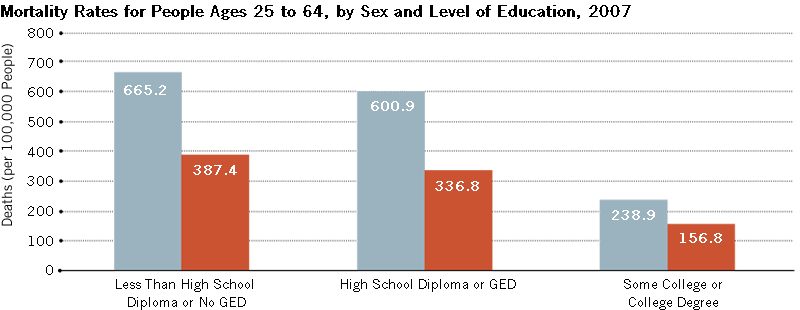
The more you learn, the more you earn! This phrase has been used by education proponents to encourage young students to stay in school or pursue higher education. But higher lifetime earnings are not the only positive outcome from increased schooling. As it turns out, the more you learn, the more you live in good health. For example, in 2007, the age-adjusted mortality rate (measured in deaths per 100,000 people) among American males between 25 and 64 years was 665.2 for individuals without a high school diploma, 600.9 for individuals who completed high school and 238.9 for individuals with some college or higher.1 In terms of healthy behaviors, the estimated incidence of smoking among American males over the age of 25 with a bachelor's degree or higher was 10.4 percent, while this figure among males with a high school degree or less was about 30 percent.2 Similar differences exist for obesity and for alcohol use.3
If more education can lead to better health, addressing the processes by which differences in education translate into differences in health can be useful to public policymakers. Identifying a causal relationship is of crucial importance in the design
of policy. For example, if more education causes better health, then policies to increase education might also be effective at improving health in the population. However, if the association (often called correlation) between education and health exists because better health allows individuals to attain a better education (reverse causation) or because the correlation between education and health results from the correlation of education with other factors that also improve health (such as income of the parents), then education-improving policies might not be effective at improving health.
Better Education=Better Behaviors
Economists David Cutler and Adriana Lleras-Muney are among those analyzing the education-related health disparities.4 The authors examine responses to the National Health Interview Survey in the United States and find a statistically significant effect of education on various measures of health, including mortality (measured as death within five years of the survey) and incidence of common acute and chronic diseases (such as heart condition, stroke, hypertension, high cholesterol, diabetes, asthma and so on). The authors report that more-educated people are less likely to suffer from these diseases. Interestingly, some common diseases, such as cancer, do not seem to exhibit an effect from education (which indicates that incidence does not vary with education).5
A major reason for the differences in health outcomes is, not surprisingly, differences in healthy behaviors. For example, in the United States, the incidence of smoking, obesity and heavy drinking is lower among the better educated.6 More-educated people are more likely to exercise and obtain preventive care (flu shots, vaccines, mammograms). More-educated people are also more likely to use seat belts and have smoke detectors in the house.
Differences in behavior, however, do not explain all the differences in health outcomes by education, but they do explain a significant proportion: Cutler and Lleras-Muney find that the effect of education on mortality is reduced by 30 percent when they control for exercise, smoking, drinking, seat belt use and use of preventive care.
Income, Information
Cutler and Lleras-Muney consider several alternative mechanisms for why education affects health. Perhaps the most obvious factor to explain difference in health outcomes would be differences in income. More education generally leads to higher income, which, in turn, allows for better access to better health care. However, they argue that it is unlikely that income and health care can account entirely for the association between education and health as many of the behaviors they analyze occur independent of health-care access. The authors estimate that differences in income account for about 20 percent of the impact of higher education on health behaviors. Price differences are also unlikely to be an important determinant, considering that unhealthy behaviors such as smoking, drinking and overeating are costly but are, nevertheless, more prevalent among less-educated individuals.
An interesting theory developed by Cutler and Lleras-Muney is that education provides individuals with better access to information and improves critical thinking skills.7 What this means is that people with more education tend to be better-informed and make better use of the information they acquire when making health-related decisions. These attributes of education are, in turn, reflected in health-related choices. For example, people with more education seem to understand more clearly the dangers of smoking, are more likely to be informed about new drugs or complex medical procedures and seem to better understand discharge instructions after emergency room visits. The authors estimate that cognitive skills account for up to 30 percent of the education effect on health behaviors.
Passing Good Health on to Children
On top of its association with adult health, greater educational attainment also promotes the transmission of health from parents to children. Economist Janet Currie provides a recent overview of the economics literature addressing two ways this occurs. First, she finds evidence that parental socio-economic status (measured by income or education) has a strong relationship with childhood health. The reasons for this are very intuitive. Wealthier families can afford better quality health care and general consumption that promotes better health (better food, safer toys and so on). Children of poorer families, in contrast, tend to suffer more adverse health shocks than children of richer families; the former also recover more slowly. In the case of chronic diseases, such as asthma, poorer children are less likely than richer children
to manage their condition properly.
Second, she finds strong evidence that childhood health plays an important role in future outcomes. In fact, some economists believe the observed relationship between income and health in adulthood may have its roots in childhood.8 Currie reports that in developing countries there is a lot of evidence indicating that individuals with poor health during childhood also tend to achieve lower education levels later in life. A similar relationship is found in developed countries; in particular, low weight at birth (a strong predictor of childhood health) has been associated with lower future test scores, educational attainment levels, wages and probabilities of being employed.
Understanding the role of health in the intergenerational transmission of socio-economic status is a promising avenue for policy. Currie notes that the evidence supporting a causal relationship between parental socio-economic status and child health and a causal relationship between child health and future outcomes is for now still limited. As noted earlier, distinguishing between simple correlation and causality is important for designing effective public policy. If parental socio-economic status does not impact child health, then public policies aimed at improving socio-economic status of the parents will not necessarily improve their children's health.
Mortality Rates for People Ages 25 to 64, by Sex and Level of Education, 2007
{kind=link}
SOURCE: National Vital Statistics Report, 2007
NOTE: Data are for 22 reporting states and the District of Columbia that use the 2003 version of the U.S. Standard Certificate of Death. Data for states that use the 1989 version of the U.S. Standard Certificate of Death, which classifies educational attainment by years of schooling instead of level, exhibit the same trend.
Endnotes
- See National Center for Health Statistics, 2010a. [back to text]
- See National Center for Health Statistics, 2010b. [back to text]
- See Cutler and Lleras-Muney, 2010. [back to text]
- See Cutler and Lleras-Muney, 2006, 2010. [back to text]
- The authors use self-reports of the incidence of disease as opposed to objective measures (doctor diagnosis). For some of the more serious diseases considered, such as heart conditions and cancer, self-reports would indicate that individuals have been already diagnosed, however. [back to text]
- Cutler and Lleras-Muney report that each additional year of education is associated with a reduction in the probability of smoking of 3 percentage points, a reduction in the probability of being obese of 1.4 percentage points and a reduction in the probability of being a heavy drinker (defined as drinking an average of five or more drinks when a person drinks) of 1.8 percentage points. [back to text]
- The most common of these cognitive skills the authors consider is reading. [back to text]
- Economists Anne Case, Darren Lubotsky and Christina Paxson find that gap in childhood health status between children of low socio-economic status and high socio-economic status grows with age. Children from lower income families enter adulthood with both lower socio-economic status and poorer health. [back to text]
References
Case, Anne; Lubotsky, Darren; and Paxson, Christina. "Economic Status and Health in Childhood: The Origins of the Gradient." American Economic Review, December 2002, Vol. 92, No. 5, pp. 1,308-34.
Currie, Janet. "Healthy, Wealthy, and Wise: Socioeconomic Status, Poor Health in Childhood, and Human Capital Development." Journal of Economic Literature, March 2009, Vol. 47, No. 1, pp. 87-122.
Currie, Janet; and Hyson, Rosemary. "Is the Impact of Health Shocks Cushioned by Socioeconomic Status? The Case of Low Birthweight." American Economic Review, March 1999, Vol. 89, No. 2, pp. 245-50.
Cutler, David M.; and Lleras-Muney, Adriana. "Education and Health: Evaluating Theories and Evidence." National Bureau of Economic Research (NBER) Working Paper No. 12352, June 2006.
Cutler, David M. and Lleras-Muney, Adriana. "Understanding Differences in Health Behaviors by Education." Journal of Health Economics, January 2010, Vol. 29, No. 1, pp. 1-28.
National Center for Health Statistics. "Deaths: Final Data for 2007." National Vital Statistics Reports, Vol. 58., No. 19. Hyattsville, Md.: May 20, 2010a. Table 26. See www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_19.pdf
National Center for Health Statistics. "Health, United States, 2009: With Special Feature on Medical Technology." Hyattsville, Md.: January 2010b. Table 61. See www.cdc.gov/nchs/data/hus/hus09.pdf
Views expressed in Regional Economist are not necessarily those of the St. Louis Fed or Federal Reserve System.
For the latest insights from our economists and other St. Louis Fed experts, visit On the Economy and subscribe.
Email Us